
Epistaxis Management - First Aid
EpistaxisUse this resource in conjunction with your real-world training

Experience Summary
This series was developed with Liverpool University Hospitals to increase understanding of the management of epistaxis. In this 360-degree video, observe the first aid management of epsitaxis.
Clinical Context
Epistaxis, commonly referred to as a nosebleed, is a frequent clinical presentation that ranges from mild self-limiting bleeds to severe, life-threatening hemorrhages. It accounts for approximately 10% of ENT emergency visits. Epistaxis can occur at any age but shows bimodal peaks in children (typically due to trauma or nasal dryness) and the elderly (often linked to hypertension, anticoagulant use, or coagulopathies).
Nasal bleeding is typically categorised anatomically into anterior and posterior epistaxis. Anterior bleeds originate from Kiesselbach's plexus (Little's area) on the anterior nasal septum and account for approximately 90% of cases. Posterior bleeds, arising from branches of the sphenopalatine artery, are less common but more severe, often requiring specialist intervention.
Stepwise Management of Epistaxis
- Initial Assessment and ResuscitationThe first priority is to assess the patient’s airway, breathing, and circulation (ABC). In cases of significant bleeding, establish intravenous access, initiate fluid resuscitation, and monitor vital signs. Oxygen may be provided if required. Continuous bleeding with hemodynamic instability warrants urgent intervention.
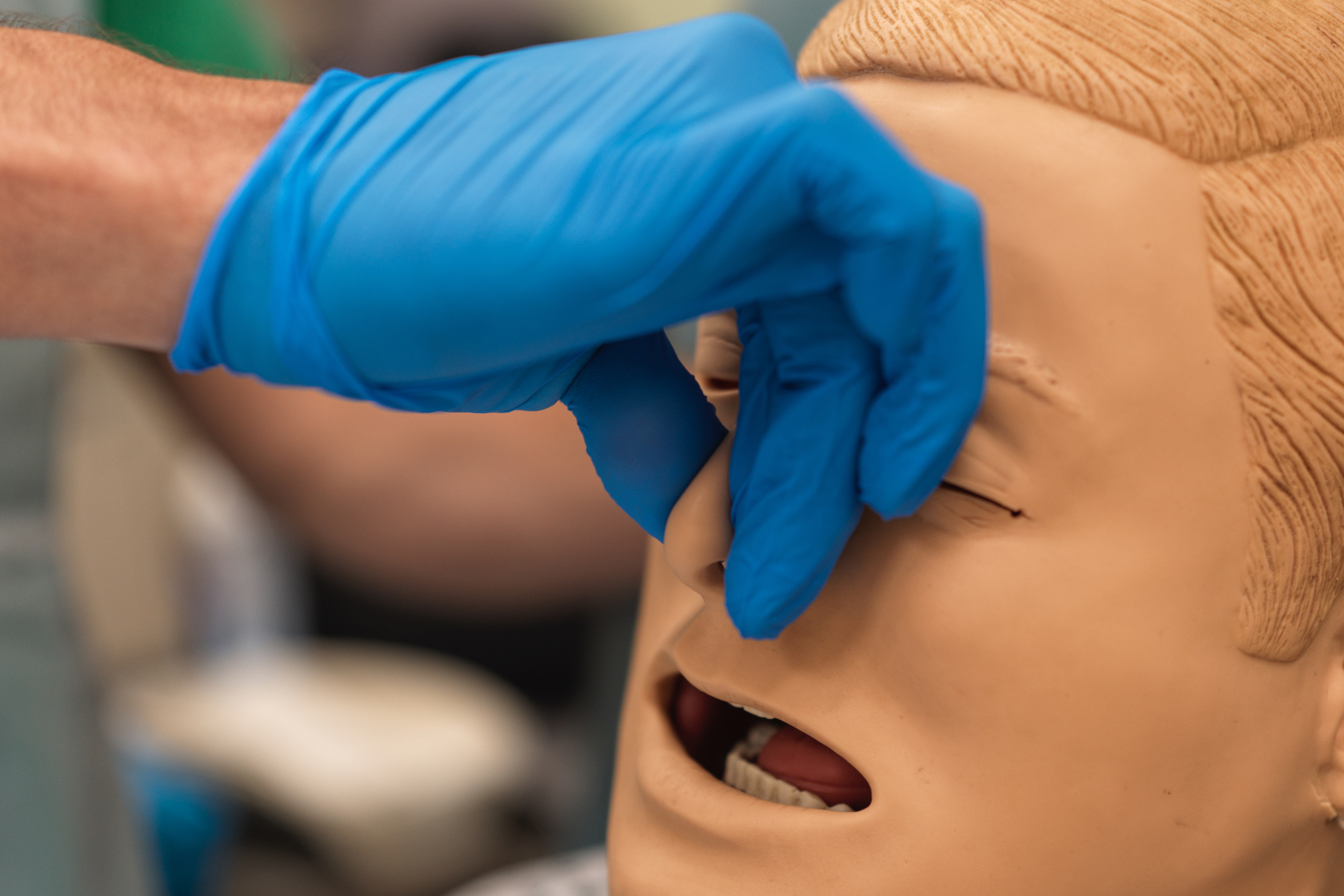
- First Aid MeasuresFor most cases, simple first aid is effective. The patient should be positioned sitting upright with the head tilted slightly forward to prevent aspiration of blood. The soft part of the nose should be pinched firmly for 10-15 minutes. Cold compresses to the nasal bridge may also help by vasoconstriction.
- Nasal ExaminationOnce bleeding has reduced or stopped, inspect the nasal cavity using a headlight and nasal speculum to identify the bleeding site. Suction may be required to clear clots. If visible, the bleeding point can be treated directly.
- CauterisationIf a bleeding point is visible, chemical cauterisation with silver nitrate or electrical cautery may be performed. Care must be taken to avoid bilateral septal cautery, which risks septal perforation.
- Nasal PackingIf bleeding persists, nasal packing is indicated. Anterior nasal packing can be performed using Merocel sponges, anterior nasal packs, or ribbon gauze soaked in antiseptic. For posterior epistaxis, posterior nasal packing with a Foley catheter or commercial balloon device may be necessary.
- Surgical and Interventional OptionsRefractory cases may require surgical ligation of the sphenopalatine artery or endovascular embolization, especially for posterior bleeds.
- Identify and Treat Underlying CausesA thorough history is essential to identify factors such as trauma, coagulopathies, hypertension, anticoagulant use, or nasal tumors that may contribute to recurrent or severe epistaxis. Addressing these is vital to prevent recurrence.
Learning Outcomes
- Understand the first aid management for epistaxis.
- Understand the technique for digital pressure on the nose.
- Revise the common pitfalls and myths around epistaxis first aid.
External Resources